

by Lance Hadley and Aniket Bhushan
Updated: July 23, 2019
On June 4th, at the Women Deliver conference in Vancouver, Prime Minister Justin Trudeau announced a C$1.4billion annual commitment to support women and girls’ health around the world starting in 2023, with half the amount dedicated to sexual and reproductive rights (SRHR).
This analysis attempts to make sense of this commitment by raising two questions:
- How does this historic C$1.4billion annual commitment compare to similar past commitments?
- How does it comport with trends in global health spending, and overall trends in international assistance spending?
How does the C$1.4billion annual spending commitment compare to similar past commitments?
The C$1.4billion annual spending announcement made at the Women Deliver conference has been rightly lauded by civil society organizations as “historic”.
Given it is a 10-year commitment, this is a significant achievement in terms of increasing the predictability of international assistance spending on women and girls’ health.
It also clearly prioritizes a high return on investment area in development spending, as it is widely acknowledged that spending on women and girls’ health (especially sexual rights) can have a very high development payoff in terms equity, empowerment and wider macroeconomic effects such as accelerating the demographic dividend.
This commitment builds on a longstanding Canadian development priority:
Muskoka/MNCH 1.0; 2010-2015; C$2.85billion; Conservative – PM Harper
The first significant spending commitment on women and girls’ health was made under the Conservative government of Stephen Harper at the 2010 G7/8 summit Canada hosted in Muskoka. This commitment to maternal newborn child health (MNCH), which came to be known as the Muskoka Initiative, was a 5year C$2.85billion commitment, a level that was exceeded in the final tally (according to our analysis the actual total spending reached C$3.12billion over 5 years).
On an annual basis, core health sector spending ranged between $500mn to C$670mn during this period (spending on reproductive health and population policies during this period was additional, approx. C$200mn-250mn annually).
MNCH 2.0; 2015-2020; C$3.5billion – Started by Conservatives, retained and built on by the Liberals
In 2014, the then Conservative government under PM Harper announced an extension and expansion, whereby Canada committed to spend C$3.5billion on MNCH from 2015 to 2020. When the Liberals took over in 2015, they retained this commitment and expanded it further (by covering the full spectrum of reproductive and sexual health and rights, including abortion).
During this period (2015-2018) core health spending ranged between C$600mn to $750mn annually. Spending on reproductive and population health (the best available proxy for SRHR) expanded much faster, from approx. C$200mn annual at the start of the period to approx. C$345mn by 2017-18.
Relative to past similar commitments, the C$1.4billion annual spending announcement represents a significant increase; nearly double the level compared to MNCH 1.0 and 30% to 40% higher compared to MNCH 2.0 on an annual basis.
How does it comport with trends in Canada’s global health spending and overall international assistance spending?
The above analysis only provides a partial assessment for two reasons: first, we know that both health spending and gender-targeted spending is growing rapidly and expected to grow further; given both the explicit target of 95% gender focused spending of the Feminist International Assistance Policy and international obligations (e.g. commitments to multilaterals which account for a significant share of Canada’s global health spending at approx. 70%). Second, sector-specific spending is partly a function of overall international assistance spending, which again is growing and expected to grow further, even if only modestly.
A proper assessment of the level of ambition of the C$1.4billion annual commitment would need to consider recent and expected trends in both health sector and overall assistance levels.
Furthermore, the recent announcement is vague in specifying what is and isn’t being counted towards the C$1.4billion annual figure.
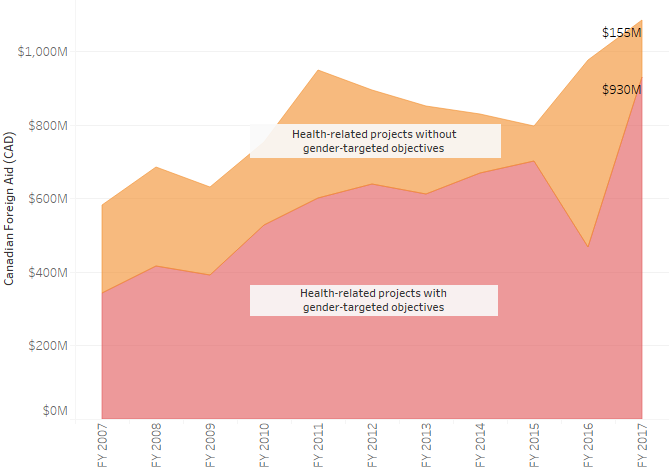
With the above caveats in mind and in order to fill the gap in understanding, below we define spending on women and girls’ health by aggregating spending coded to the OECD-DAC sectors: health and population policies/programmes & reproductive health. We also reflect the gender-targeting level. We leverage project-level open data, sourced from the Historical Project Data Set (HPDS) which is freely available via our Platform on multiple levels. The data in the graphics below are reflective of all Canadian departments and agencies providing assistance (data on our projects explorer tool is reflective of GAC only).
Our main findings at the sector level are as follows:
- In fiscal year 2017-18, Canada spent approx. C$1.1 billion on health-related projects. Approx. 85% or C$930mn of this spending was gender-targeted (gender marker 1, 2, or 3).
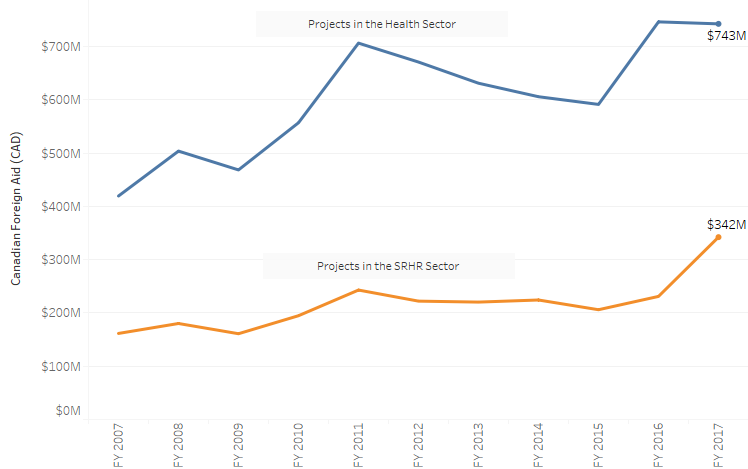
- For fiscal 2017-18, total core health sector spending was approx. C$743mn while spending on SRHR was approx. C$342mn.
- SRHR has been the main driver of increases in health spending in recent years; SRHR spending in 2017-18 was almost 50% higher compared to the previous year.
- Over the past 10 years, since 2007, total health spending (inclusive of reproductive health) has grown at a CAGR of approx. 6.5%. The CAGR over the last 5 years (since the peak in 2012 after which there was a drop) is approx. 4%.
As mentioned, sector level trends are partly a function of overall trends in assistance. To this end we can reflect on the main source of Canadian aid spending, which is the International Assistance Envelope (IAE).
To do this we leverage recent Budget documents (fiscal measures tables) and GAC’s statistical reports to Parliament. Budget 2018 and 2019 are important as they lay out the fiscal profile of additions to the envelope since the adoption of the new Feminist assistance policy. This is reflected in the first table below.
The second table reflects IAE levels, both, as reported to Parliament (programs funded by the IAE, across department) and as represented in the IAE structure detailed in recent Budgets. An important caveat to keep in mind here is that while the reports to Parliament are on an ex-post expenditure basis, the IAE structure detailed in Budgets 2018 and 2019 are on an ex-ante budgetary allocation basis. Admittedly this is not an apples to apples comparison (as a lot of factors affect budgeting vs. actual expenditure, e.g. level of unused IAE room, if and how it is carried forward from year to year, level of sun-setting projects, launch of new initiatives etc). However it is the best we can do with available data. Starting in 2020 GAC will issue a new consolidated report on the IAE which is expected to present actual expenditures against budgets more clearly as relates to the IAE account.
Based on the available data, our estimations have significant implications for the what this new commitment means for Canadian development spending:
- If we assume the IAE level at approx. C$4.9bn in 2015 (accounting for certain exceptional double payments etc. that affected figures at the time), and assume that it reaches the C$5.7bn level projected for 2019 in the most recent Budget, this implies a CAGR of approx. 3.85%
- Our estimate for the IAE level in 2023-24 based on figs in the tables below and a set of assumptions (beyond the purview of the discussion here) is approx. C$6.1billion. Relative to current actual IAE expenditure levels (2017-18) this would represent a CAGR of approx. 3.1%
- These figures are important because the announced commitment only begins in 2023. If we assume that health spending maintains its share in overall assistance spending and we assume the overall envelope trends as estimated, we estimate that from 2017-18 out to 2023-24 Canada’s health spending will grow in the range of CAGR 3.2% to 4%
- If we apply this to the present known level of health spending (C$1.1billion in 2017-18) the corresponding level (all else equal) by 2023 would be around C$1.31billion to C$1.37billion
- In other words, Canada’s health spending by 2023, when the commitment is supposed to begin for 10years, will already be very close to the C$1.4billion commitment announced.
- This somewhat changes the picture. While on the face of it the commitment looks like a substantial increase (doubling) relative to past similar commitments. A deeper look, given what we know about the trend in health spending and expected future spending given announced increments between the present and 2023, shows that this announcement is more a reconfirmation of health spending than a substantial increase.


Conclusion
The aim of this analysis has been to put into perspective Canada’s commitment to spend $1.4billion annually, for 10 years, on women and girls’ health starting in 2023, which was announced at the Women Deliver conference in June 2019. We do so in two ways: first, by comparing this announcement to past similar commitments. Second, by providing a forward looking analysis based on recent trends in health and gender related spending, and expected trends in the IAE given what we know about planned increments out to 2023, when this commitment is supposed to begin.
Our main findings are as follows:
- On face value, relative to past similar commitments, the C$1.4billion annual spending announcement represents a significant increase; nearly double the level compared to MNCH 1.0 and 30% to 40% higher compared to MNCH 2.0 on an annual basis.
- Given it is a 10 year commitment, this is a significant achievement in terms of increasing the predictability of international assistance. It also prioritizes a high return high impact area in development spending.
- However we know that health (and gender related) spending are growing and expected to grow further, given the adoption of the FIAP.
- We also know that the overall envelope (IAE) is expected to grow, even if only modestly.
- We estimate that out to 2023-24, the IAE will grow at approx 3.1% CAGR.
- Furthermore, we demonstrate that the IAE has already been growing (since 2015, at approx 3.85% CAGR); and that health spending has been growing (at 6.5% CAGR over 10 years since 2007 and 4% since its peak in 2012).
- In order to stay in line with recent trends and roughly maintain its share in a modestly growing envelope, we estimate that health spending will quite naturally grow at between 3.2% to 4% CAGR out to 2023 when this commitment is expected to begin. This of course is based on a number of assumptions (all of which, in our view, are fairly conservative; i.e. if anything growth could be even faster as has been the case in certain areas of health spending, notably SRHR under the Liberal government).
- We demonstrate that the current level of core health and SRHR spending (using reproductive health as our proxy) is already around $1.1 billion annual.
- If we apply our estimated growth range (between 3.2% to 4% CAGR) to this, all else being equal, health spending to be in the range of $1.31 billion to $1.37 billion annually by 2023.
- Since this level is very close to the $1.4 billion annual level announced, we conclude that this commitment is more a reconfirmation than a substantial increase.
- It may also be qualitatively different from past similar commitments for two reasons. Nothing prevents a new government (or the same government) from changing this, both since it begins further out in time (2023), and because it is unclear if any additional resources required to meet the commitment level have been added to the IAE profile or if they remain to be negotiated in the future. This is different from the past two health sector commitments which were made largely out of existing IAE resources at the time.
Related Resources
Canadian Gender Targeted Spending
Gender Targeted ODA – Comparative DAC Donor Analysis
Canadian Official Development Assistance Addressing Sexual and Gender Based Violence
FIAP and Sub-Saharan Africa: Ambitious New Target?
How Canada can leverage its new Equality Fund to lead on women’s empowerment
Recent Comments